Nursing Diagnosis: Risk for Impaired Gas Exchange related to changes in alveolar capillary membrane due to a buildup of fluid in the lung cavity
Purpose:
After nursing actions on the client, with the expected outcomes:
Looks adequate ventilation and oxygenation of the tissues in which normal limits, and free from symptoms of respiratory distress.
Participate in treatment.
Interventions:
Auscultation breath sounds, note the wheezing.
Teach the client to cough effectively and breathe deeply.
Adjust the position of sleeping with the head elevated 200-300, semi-Fowler, put a pillow on the elbow.
Give medications as indicated.
Provide oxygen as needed.
Rational:
Indicate the presence of congestive lung / collection secretion.
Clearing the airway and facilitate the exchange of oxygen.
Reducing the need for oxygen and improve lung development to the fullest.
Increasing the concentration of oxygen alveoli, which may reduce tissue hypoxemia.
Bronchodilator, increase oxygen intake by widening the airway and commercialize a diuretic effect on the reduction of pulmonary failure.
Nursing Diagnosis: Risk for Suicide Application of NANDA, NOC, NIC
Nursing Diagnosis: Risk for Suicide Gail B. Ladwig
NANDA Definition: At risk for self-inflicted, life-threatening injury
Related Factors:
Behavioral
History of previous suicide attempt; impulsiveness; buying a gun; stockpiling medicines; making or changing a will; giving away possessions; sudden euphoric recovery from major depression; marked changes in behavior, attitude, school performance
Verbal
Threats of killing oneself; states desire to die/end it all
Situational
Living alone; retired; relocation, institutionalization; economic instability; loss of autonomy/independence; presence of gun in home; adolescents living in nontraditional settings (e.g., juvenile detention center, prison, half-way house, group home)
Psychological
Family history of suicide; alcohol and substance use/abuse; psychiatric illness/disorder (e.g., depression, schizophrenia, bipolar disorder); abuse in childhood; guilt; gay or lesbian youth
Demographic
Age: elderly, young adult males, adolescents; race: Caucasian, Native American; gender: male divorced, widowed
Physical
Physical illness; terminal illness; chronic pain
Social
Loss of important relationship; disrupted family life; grief, bereavement; poor support systems; loneliness; hopelessness; helplessness; social isolation; legal or disciplinary problem; cluster suicides
NOC Outcomes (Nursing Outcomes Classification)
Suggested NOC Labels
·Cognitive Ability
·Depression Control
·Distorted Thought Control
·Impulse Control
·Self-Mutilation Restraint
·Suicide Self-Restraint
·Will to Live
Client Outcomes
·Does not harm self
·Expresses decreased anxiety and control of hallucinations
·Talks about feelings; expresses anger appropriately
·Obtains no access to harmful objects
·Yields access to harmful objects
NIC Interventions (Nursing Interventions Classification)
Suggested NIC Labels
·Anxiety Reduction
·Coping Enhancement
·Crisis Intervention
·Suicide Prevention
·Surveillance
Nursing Interventions and Rationales
·Establish a therapeutic relationship with client This study demonstrated the importance of this relationship in identifying and preventing suicide (Rudd et al, 2000).
·Monitor, document, and report client's potential for suicide. Traits such as impulsivity, poor social adjustment, and mood disorders are associated with adolescent suicide attempts (Brent et al, 1994).
·Be alert for warning signs of suicide:
oVerbalizations such as, "I can't go on," "Nothing matters anymore," "I wish I were dead"
oBecoming depressed or withdrawn
oBehaving recklessly
oGetting affairs in order and giving away valued possessions
oShowing a marked change in behavior, attitudes, or appearance
oAbusing drugs or alcohol
oSuffering a major loss or life change
Suicide is rarely a spur-of-the-moment decision. In the days and hours before people kill themselves, there are usually clues and warning signs (Befrienders International, 2001).
·Assess for suicidal ideation when the history reveals:
oDepression
oAlcohol or other drug abuse
oOther psychiatric disorder
oAttempted suicide
oRecent divorce and/or separation
oRecent unemployment
oRecent bereavement
oChronic pain
Clinicians should be alert for suicide when the above factors are present in asymptomatic persons (National Guideline Clearing House, 2001). This study revealed that clients with chronic pain and depression expressed suicidal ideation (Fisher et al, 2001). The process leading to suicide in young people is often untreated depression (Houston, Hawton, Shepperd, 2001).
·Refer to mental health counseling and possible hospitalization if there is evidence of suicidal intent, which may include evidence of preparatory actions (e.g., obtaining a weapon, making a plan, putting affairs in order, giving away prized possession, preparing a suicide note).
·Question family members regarding the preparatory actions mentioned. Clinicians should be alert for suicide when these factors are present in asymptomatic persons (National Guideline Clearing House, 2001).
·Refer family members and friends to local mental health agencies and crisis intervention centers if client has suicidal ideation or there is a suspicion of suicidal thoughts. Clients at risk should receive evaluation and help (National Guideline Clearing House, 2001).
·Consider outpatient commitment for actively suicidal client. Involuntary outpatient commitment can improve treatment, reduce the likelihood of hospital readmission, and reduce episodes of violent behavior in persons with severe psychiatric illnesses (Torrey, Zdanowicz, 2001).
·Counsel parents and homeowners to restrict unauthorized access to potentially lethal prescription drugs and firearms within the home. Identifying teens at high risk of firearm suicide and limiting access to firearms is a type of public health intervention likely to be successful in preventing firearm suicides (Shah, Hoffman, Wake, Marine, 2000).
·See care plan for Risk for self-directed Violence.
Multicultural
·Assess for the influence of cultural beliefs, norms, and values on the individual's perceptions of suicide. What the individual believes about suicide may be based on cultural perceptions (Leininger, 1996).
·With the client's consent, facilitate family-oriented crisis intervention. Family-oriented crisis intervention can clarify stresses and allow assessment of family dynamics (Baker, 1988).
·Facilitate modeling and role-playing for client and family regarding healthy ways to start a discussion about the client's suicide attempt. It is helpful for families and the client to practice communication skills in a safe environment before trying them in a real-life situation (Rivera-Andino, Lopez, 2000).
·Identify and acknowledge the stresses unique to culturally diverse individuals. Financial difficulties and maintaining cultural values are two of the most common family stressors cited by women of color (Majumdar, Ladak, 1998).
·Encourage the family to demonstrate and offer caring and support to each other. The familial characteristics of care and support may be associated with fostering resiliency in African-American families. Resilience is the ability to experience adverse conditions and successfully overcome them (Calvert, 1997).
·Validate the individual's feelings regarding concerns about current crisis and family functioning. Validation lets the client know that the nurse has heard and understands what was said, and it promotes the nurse-client relationship (Stuart, Laraia, 2001; Giger, Davidhizer, 1995).
Nursing Care Plan for C-section - Nursing Diagnosis for Cesarean section (C-section)
Cesarean Section or C-section is a surgery carried out to deliver a baby. When there are multiple babies or any other problems, the woman is unable to have normal vaginal delivery, then her abdomen is medically cut to take the baby out. Mostly C-section is operated when unexpected complications occur during delivery. These can be:
Health problems in mother that might be long-term
Abnormal position of the fetus
Congested room for the baby to go through vagina
Any defects in the baby
Carrying more than one baby
It is generally safe for both mother and baby but is a major surgery with many risks. Moreover, recovery takes a long time than in normal delivery.
Nursing Diagnosis for Cesarean section (C-section)
Gastroenteritis is a swelling of the lining of the stomach and intestines, frequently accompanied with acute diarrhea and vomiting, mild fever and stomach cramps. Gastroenteritis attacks can take from anywhere between six hours to 3 days to pass. Symptoms ordinarily are caused by toxins produced by bacteria in the food or by a swelling of the intestine through having a virus or bacteria being present. Ordinarily, food poisoning results in a much quicker onset of symptoms, which can strike the sufferer within the hour of eating infected foods.
Gastroenteritis is frequently connected with diarrhea given it occurs most often in the home ordinarily resulting from poor hygiene. Pre-cooked meats particularly chicken, raw egg dishes and shellfish are the most frequent causes of bacterial and viral gastroenteritis. Further culprits include foods which are past their sell by dates. Seafood's and to some extent dairy products, often smell bad when they have gone off, but this does not always the case with other foods. It is therefore extremely important to store food correctly and always consume before its use by date.
Gastroenteritis : Causes, Symptoms, and Management
Gastroenteritis, commonly known as the stomach flu, is an inflammation of the gastrointestinal tract characterized by symptoms like diarrhea, abdominal cramps, nausea, and vomiting. While typically a self-limiting condition, understanding its causes, symptoms, and appropriate management is essential for timely recovery.
Causes:
Gastroenteritis is often triggered by viral or bacterial infections. Viruses such as norovirus, rotavirus, and adenovirus are common culprits, especially in cases affecting children. Bacterial infections may result from consuming contaminated food or water, with pathogens like Salmonella, Escherichia coli (E. coli), and Campylobacter being frequent causes.
Symptoms:
The hallmark symptoms of gastroenteritis include diarrhea, which can be watery or contain blood, abdominal cramps, nausea, and vomiting. Individuals may also experience fever, headache, and muscle aches. Symptoms can manifest suddenly and vary in severity, with dehydration being a potential concern, particularly in cases of persistent vomiting and diarrhea.
Management:
Fluid Replacement: One of the primary concerns with gastroenteritis is dehydration due to fluid loss. Rehydration is crucial, and oral rehydration solutions or, in severe cases, intravenous fluids may be recommended.
Dietary Modifications: While the stomach is recovering, a temporary shift to a bland diet may be beneficial. This often includes easily digestible foods like bananas, rice, applesauce, and toast (BRAT diet).
Probiotics: Probiotics, found in yogurt or available as supplements, may help restore the balance of beneficial bacteria in the gut, aiding in recovery.
Antimicrobial Medications: In cases caused by bacterial infections, antimicrobial medications may be prescribed. However, these are typically reserved for specific instances, as indiscriminate use can contribute to antibiotic resistance.
Symptomatic Treatment: Over-the-counter medications may be used to alleviate symptoms such as fever, pain, or nausea. However, their use should be guided by healthcare professionals.
1. Guarino, A., Ashkenazi, S., Gendrel, D., Lo Vecchio, A., Shamir, R., & Szajewska, H. (2014). European Society for Pediatric Gastroenterology, Hepatology, and Nutrition/European Society for Pediatric Infectious Diseases evidence-based guidelines for the management of acute gastroenteritis in children in Europe: update 2014. Journal of Pediatric Gastroenterology and Nutrition, 59(1), 132-152. doi: 10.1097/MPG.0000000000000375
2. Riddle, M. S., DuPont, H. L., & Connor, B. A. (2016). ACG Clinical Guideline: Diagnosis, Treatment, and Prevention of Acute Diarrheal Infections in Adults. American Journal of Gastroenterology, 111(5), 602–622. doi: 10.1038/ajg.2016.126
Nursing Diagnosis for Self-Care Deficit - Bathing / Hygiene
Definition
Circumstances where individuals have failed to implement or complete ability bathing / hygiene activities.
Data:
Lack of ability to bathe themselves (including washing the whole body, combing hair, brushing teeth, doing skin care and nails as well as the use of makeup)
Can not or no desire to wash the body or body parts.
Can not use the source water.
Inability to feel the need for hygiene measures.
Lack of ability to wear his own clothes (including underwear routine or special clothing, not the clothes the night)
Failure of the ability to use or release of clothes.
Inability to fasten clothing.
Inability to dress themselves satisfactorily.
Expected outcomes are:
Individuals will
1. Identifying the love of self-care activities.
2. Demonstrated that optimal hygiene in care after assistance is given.
3. Participate in physical and or verbal self-care activities
Carry out the shower activity at its optimal level.
Reported satisfaction with the achievements despite the limitations.
Connecting a feeling of comfort and satisfaction with the cleanliness of the body.
Demonstrate ability to use adaptive assistive devices.
Describe the factors that cause of the lack of ability to bathe.
Nursing Diagnosis Excess Fluid Volume related to decreased glomerular filtration rate (decrease in cardiac output) and the retention of sodium / water.
Objectives / evaluation criteria:
Clients will be demonstrating the stable fluid volume with the balance of inputs and expenditures, breath sounds clean / clear, vital signs within an acceptable range, stable weight and no edema, fluid restriction expressed understanding of the individual.
Nursing Interventions Excess Fluid Volume :
Monitor urine output, record the number and color of the time in which diuresis occurs.
Rational: Spending a little and concentrated urine may be due to decreased renal perfusion. Supine position so that helps diuresis of urine may be increased during bed rest.
Monitor / calculate the balance of income and expenditure for 24 hours.
Rational: diuretic therapy may be caused by a sudden loss of fluid / redundant (hypovolaemia), although edema / ascites is still there.
Keep sitting or bed rest with semifowler position during the acute phase.
Rationale: The position is increasing kidney filtration thus improving diuresis.
Monitor blood pressure and CVP (if any).
Rational: Hypertension and increased CVP indicates fluid overload and may indicate an increase in pulmonary congestion, heart failure.
Assess bowel sounds. Record complaints of anorexia, nausea, abdominal distension and constipation.
Rational: visceral congestion can interfere with the function of gastric / intestinal tract.
Administration of drugs as indicated (collaboration)
Consult with the dietitian.
Rational: to provide an acceptable diet that meets client needs calories in sodium restriction.
Liver abscess is a relatively uncommon but life-threatening disorder that occurs when bacteria or protozoa destroy hepatic tissue. The damage produces a cavity, which fills with infectious organisms, liquefied hepatic cells, and leukocytes. Necrotic tissue then walls off the cavity from the rest of the liver.
A liver abscess occurs when bacteria or protozoa destroy hepatic tissue, producing a cavity, which fills with infectious organisms, liquefied liver cells, and leukocytes. Necrotic tissue then walls off the cavity from the rest of the liver. Liver abscess carries a mortality of 10% to 20%, despite treatment. Liver abscess affects both sexes and all age-groups, although it's slightly more prevalent in hospitalized children (because of a high rate of immunosuppression) and in females (most commonly those between ages 40 and 60).
Risk of infection is a nursing diagnosis which is defined as "the state in which an individual is at risk to be invaded by an opportunistic or pathogenic agent (virus, fungus, bacteria, protozoa, or other parasite) from endogenous or exogenous sources" and was approved by NANDA in 1986. Although anyone can become infected by a pathogen, patients with this diagnosis are at an elevated risk and extra infection controls should be considered.
Endogenous sources
The risk of infection depends on a number of endogenous sources. Skin damage from incision as well as very young or old age can increase a patient's risk of infection. Examples of risk factors includes decreased immune system secondary to disease, compromised circulation secondary to peripheral vascular disease, compromised skin integrity secondary to surgery, or repeated contact with contagious agents.
Assessment
The patient should be asked about a history of repeated infections, symptoms of infection, recent travel to high-risk areas, and their immunization hishttp://www.blogger.com/img/blank.giftory. They should also be assessed for objective signs such as the presence of wounds, fever, or signs of nutritional deficiency.
Intervention
The specific nursing interventions will depend on the nature and severity of the risk. Patients should be taught how to recognize the signs of infection and how to reduce their risk. Surgery is a frequent risk factor for infection and a physician may prescribe antibiotics prophylactically. Immunization is another common medical intervention for those who are at high risk for infection.
Marjory Gordon is a nursing theorist and professor who created a nursing assessment theory known as Gordon's functional health patterns. She remains the international leader in this area of nursing scholarship. Dr. Gordon served as the first president of the North American Nursing Diagnosis Association. She has been a Fellow of the American Academy of Nursing since 1977 and was named as a Living Legend by the same organization in 2009.
Academic appointment
Dr. Gordon is an emeritus professor of nursing at Boston College in Chestnut Hill, Massachusetts.
Writing and scholarship
Dr. Gordon is the author of four books, including the Manual of Nursing Diagnosis, now in its twelfth edition. Her books appear in ten different languages, in forty-eight countries and six continents.
She has contributed significantly to the development of standardized nursing language. Dr. Gordon's work in this sphere has implications for research, education, evaluation of competency, and the establishment of a core of nursing knowledge based on evidence. This language will also form the basis of the nursing component of the electronic medical record.
Education
Marjory Gordon is an alumna of the Mount Sinai Hospital School of Nursing. She earned her bachelor's and master's degrees from Hunter College of the City University of New York and her PhD from Boston College.
The self-care deficit nursing theory is a middle range nursing theory that was developed between 1959 and 2001 by Dorothea Orem. It is also known as the Orem model of nursing. It is particularly used in rehabilitation and primary care settings where the patient is encouraged to be as independent as possible.
Central philosophy
The nursing theory is based upon the philosophy that all "patients wish to care for themselves". They can recover more quickly and holistically if they are allowed to perform their own self-cares to the best of their ability.
Self-care requisites
Self-care requisites are groups of needs or requirements that Orem identified. They are classified as either:
Universal self-care requisites - those needs that all people have
Developmental self-care requisites - 1. maturational: progress toward higher level of maturation. 2. situational: prevention of deleterious effects related to development.
Health deviation requisites - those needs that arise as a result of a patient's condition
Self-care deficits
When an individual is very unable to meet their own self-care requisites, a "self-care deficit" occurs. It is the job of the Registered Nurse to determine these deficits, and define a support modality.
Support modalities
Nurses are encouraged to rate their patient's dependencies or each of the self-care deficits on the following scale:http://www.blogger.com/img/blank.gif
Total Compensation
Partial Compensation
Educative/Supportive
Universal Self-Care Requisites (SCRs)
The Universal self-care requisites that all or health are:
Air
Water
Food
Elimination
Activity and Rest
Solitude and Social Interaction
Hazard Prevention
Promotion of Normality
The nurse is encouraged to assign a support modality to each of the self-care requisites.
Risk for deficient Fluid Volume related to a sense of nausea and vomiting,
characterized by:
Sometimes diarrhea.
Abdominal distension.
Tense abdomen.
Decreased appetite.
There is a sense of nausea and vomiting.
Purpose: Maintaining the balance of fluid volume
Results Criteria:
The client is not diarrhea.
A good appetite.
The client no nausea and vomiting.
Nursing Intervention:
1) Monitor vital signs.
Rational: This is an early indicator of hypovolemia.
2) Monitor intake and urine output and concentration.
Rational: Decreased urine output and concentration will improve the sensitivity / sediment as one the impression of dehydration and require increased fluids.
3) Give fluid little by little but often.
Rationale: To minimize the loss of fluids.
That stroke is a disease affects the blood vessels That blood supply to the brain. Without blood to supply oxygen and Nutrients and to remove waste products, brain cells begin to die Quickly. Stroke is Sometimes Called a "brain attack. Stroke is a medical emergency and can cause permanent neurological damage or even death if not promptly diagnosed and treated.
The cause of stroke is an interruption in the blood supply, with a resulting depletion of oxygen and glucose in the affected area. This reduces or abolishes IMMEDIATELY neuronal function, and also initiates the ischemic cascade the which Causes neurons to die or Be Seriously Damaged, Further impairing brain function.
Kidney transplantation or renal transplantation is the organ transplant of a kidney into a patient with end-stage renal disease. Kidney transplantation is typically classified as deceased-donor (formerly known as cadaveric) or living-donor transplantation depending on the source of the donor organ. Living-donor renal transplants are further characterized as genetically related (living-related) or non-related (living-unrelated) transplants, depending on whether a biological relationship exists between the donor and recipient.
Nursing Diagnosis for Renal Transplantation
1. Risk for infection related to altered immune system secondary to immunosuppressant medications
2. Risk for altered oral mucous membranerelated to increased susceptibility to infection secondary to immunosuppression.
3. Risk for self-concept disturbancerelated to transplant experience, potential for rejection, and side effects of medications.
The most critical part of kidney transplantation is preventing rejection of the graft kidney.
Different transplant centers use different drug combinations to fight rejection of a transplanted kidney.
The drugs work by suppressing your immune system, which is programmed to reject anything "foreign," such as a new organ.
Like any medication, these drugs can have unpleasant side effects.
Some of the most common immune-suppressing drugs used in transplantation are described here.
Cyclosporine: This drug interferes with communication between the T cells of the immune system. It is started immediately after the transplant to suppress your immune system and continued indefinitely. Common side effects include tremor, high blood pressure, and kidney damage. These side effects are usually related to the dose and can often be reversed with proper dosing.
Corticosteroids: These drugs block T-cell communication as well. They are usually given at high doses for a short period immediately after the transplant and again if rejection is suspected. Corticosteroids have many different side effects, including easy bruising of the skin, osteoporosis, avascular necrosis (bone death), high blood pressure, high blood sugar, stomach ulcers, weight gain, acne, mood swings, and a round face. Because of these side effects, many transplant centers are trying to reduce the maintenance dose of the drug as much as possible or even to replace it with other drugs.
Azathioprine: This drug slows the production of T cells in the immune system.Azathioprine isusually used for long-term maintenance of immunosuppression. The most common side effects of this drug are suppression of the bone marrow, which produces blood cells, and liver damage. Many transplant centers are now using a newer drug called mycophenolate mofetil instead of azathioprine.
Newer antirejection drugs include tacrolimus, sirolimus, and mizoribin, among others. These drugs are now being used to try to reduce side effects and to replace drugs after episodes of rejection.
Other costly and experimental treatments include using antibodies to attack specific parts of the immune system to decrease its response.
In the fetus the testicle develops within the abdomen and migrates down into the scrotum, trailing its blood supply behind it like a leash. In the scrotum the testicle resides within a smooth sack called the tunica vaginalis. The testicle can spin and move about within the sack. As males grow and age the testicle develops connections with the sack making it harder for the testicle to spin or twist. This is why torsion is usually seen in younger men, adolescents, and children.
It can occur during fetal development leading to neonatal torsion or vanishing testis and is one of the main cause for monarchism (single testicle).
It needs emergency treatment to save the testicles. Other wise it can lead to permanent damage to the testicles leading to necrosis of testis and atrophy of testis. It can lead to sterility
Signs and symptoms of testicular torsion
Severe sudden pain in the scrotum.
Swelling of the scrotum.
Redness of skin of the scrotum.
Lower abdominal pain.
Fever.
Testicle is positioned at an higher level than normal or at an odd angle.
The heart pumps blood to the lungs, brain, and other organs. Interruption of the heartbeat for only a few seconds can lead to fainting (syncope) or cardiac arrest.
Fibrillation is an uncontrolled twitching or quivering of muscle fibers (fibrils). When it occurs in the lower chambers of the heart, it is called ventricular fibrillation. During ventricular fibrillation, blood is not removed from the heart. Sudden cardiac death results.
The most common cause of VF is a heart attack. However, VF can occur whenever the heart does not get enough oxygen or if a person has other heart disorders.
Conditions that can lead to VF include:
Congenital heart disease
Electrocution accidents or injury to the heart
Heart attack
Heart muscle disease, including cardiomyopathies
Heart surgery
Ischemia (lack of oxygen to the heart muscle because of narrowed coronary arteries or shock)
Sudden cardiac death (commotio cordis), typically occurring in athletes after a trauma over the surface of the heart
Most people with VF have no history of heart disease. However, many have risk factors for cardiovascular disease, such as smoking, high blood pressure, and diabetes.
Atrial fibrillation (AF) shares strong associations with other cardiovascular diseases, such as heart failure, coronary artery disease (CAD), valvular heart disease, diabetes mellitus, and hypertension. These factors have been termed upstream risk factors, but the relationship between comorbid cardiovascular disease and AF is incompletely understood and more complex than this terminology implies. The exact mechanisms by which cardiovascular risk factors predispose to AF are not understood fully but are under intense investigation. Catecholamine excess, hemodynamic stress, atrial ischemia, atrial inflammation, metabolic stress, and neurohumoral cascade activation are all purported to promote AF.
Because diabetes mellitus and obesity are increasing in prevalence and are associated with an elevated risk of AF, Fontes et al examined whether insulin resistance is an intermediate step for the development of AF. In a community-based cohort that included 279 patients who developed AF within 10 years of follow-up, no significant association was observed between insulin resistance and incident AF.
Although the precise mechanisms that cause atrial fibrillation are incompletely understood, AF appears to require both an initiating event and a permissive atrial substrate. Significant recent discoveries have highlighted the importance of focal pulmonary vein triggers, but alternative and nonmutually exclusive mechanisms have also been evaluated. These mechanisms include multiple wavelets, mother waves, fixed or moving rotors, and macro-reentrant circuits. In a given patient, multiple mechanisms may coexist at any given time. The automatic focus theory and the multiple wavelet hypothesis appear to have the best supporting data. Automatic focus
A focal origin of AF is supported by several experimental models showing that AF persists only in isolated regions of atrial myocardium. This theory has garnered considerable attention, as studies have demonstrated that a focal source of AF can be identified in humans and that isolation of this source can eliminate AF.
The pulmonary veins appear to be the most frequent source of these automatic foci, but other foci have been demonstrated in several areas throughout the atria. Cardiac muscle in the pulmonary veins appears to have active electrical properties that are similar, but not identical, to those of atrial myocytes. Heterogeneity of electrical conduction around the pulmonary veins is theorized to promote reentry and sustained AF. Thus, pulmonary vein automatic triggers may provide the initiating event, and heterogeneity of conduction may provide the sustaining conditions in many patients with AF. Multiple wavelet
The multiple wavelet hypothesis proposes that fractionation of wave fronts propagating through the atria results in self-perpetuating "daughter wavelets." In this model, the number of wavelets is determined by the refractory period, conduction velocity, and mass of atrial tissue. Increased atrial mass, shortened atrial refractory period, and delayed intra-atrial conduction increase the number of wavelets and promote sustained AF. This model is supported by data from patients with paroxysmal AF demonstrating that widespread distribution of abnormal atrial electrograms predicts progression to persistent AF. Intra-atrial conduction prolongation has also been shown to predict recurrence of AF. Together, these data highlight the importance of atrial structural and electrical remodeling in the maintenance of AF—hence the phrase "atrial fibrillation begets atrial fibrillation."
Fibrillation is an arrhythmia that affects either the atria as a pair, or the ventricles as a pair, producing “a-fib”, or “v-fib”, respectively. (Come to think of it, if a person is in VF, do their atria fibrillate as well? Does it matter?) Most cardiac rhythms are organized – they’re regular in some way, producing some sort of regular (as opposed to disorganized), rhythmic motion of the chambers, hopefully producing a blood pressure. In fibrillation, the cardiac tissue of the chambers involved wiggles about like (classic phrase) “a bag of worms”. Does a chamber wiggling like a bag of worms pump any blood, produce a cardiac output, eject any fraction of its contents? No, it does not!
As I always try to point out, all the waves that you see on EKG strips actually represent some kind of physical motion of one or the other set of cardiac chambers, and the trick is to try to visualize what those chambers are doing in any given rhythm situation. Let’s see if a quick review of some strips helps the visualization process. Can I have the first slide please?
Here we are: look familiar? Sinus rhythm. Organized, rhythmic, producing stable contraction of the chambers – first the atria, then the ventricles. So - visualizing on the mental screen, that’s what I see: nice orderly motion, first above, then below.
Okay so far? Right – next slide, please. OK: atrial flutter. Still organized: the atria are contracting rapidly, sure, at about 300 bpm, and the ventricles are responding to every third or fourth impulse, slowly enough that the ventricular chambers have time to fill up nicely between beats, fast enough to probably maintain a good blood pressure. So I visualize the atria clipping along, with the ventricles contracting every third or fourth time.
This one? Well – is it organized? Actually it is: see the pattern of doubles? It’s a little easier to figure out by looking at the lower part of the strip – this is a sinus rhythm, and after every sinus beat comes a PAC, followed by a compensatory pause. So yes, still organized. “Regularly irregular”.
How about this one? Yup, VT. Ugly, scary, but still organized, regular – the chambers (which ones?) are moving in a steady manner. On your mental screen you should see the ventricular walls contracting very rapidly – do they have time to fill? Should we shock this rhythm? It depends…
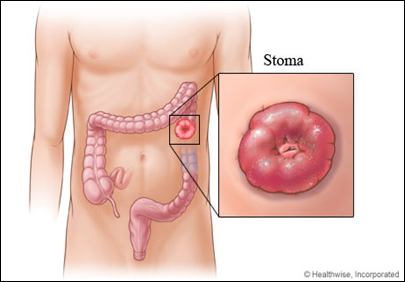
Colostomy is a surgical procedure that brings one end of the large intestine out through the abdominal wall. Stools moving through the intestine drain into a bag attached to the abdomen.
Description
The procedure is usually done after:
Bowel blockage (obstruction)
Bowel resection
Injuries
The colostomy may be short-term or permanent.
Colostomy is done while you are under general anesthesia (asleep and pain-free). It may either be done with a large surgical cut in the abdomen, or with a small camera and several small cuts (laparoscopy).
The type of approach used depends on what other procedure done needs to be done. In general, the surgical cut is made in the middle of the abdomen. The bowel resection or repair is done as needed.
Nursing Care Plan for Colostomy
Sample Nursing Diagnosis for Colostomy
1. Risk for Impaired Skin Integrity : risk factors may include absence of sphincter at stoma and chemical irritation from caustic bowel contents, reaction to product/removal of adhesive, and improperly fitting appliance.
2. Risk for Diarrhea/Constipation : risk factors may include interruption/alteration of normal bowel function (placement of ostomy), changes in dietary/fluid intake, and effects of medication.*
3. Deficient Knowledge [Learning Need] regarding changes in physiologic function and self care/treatment needs may be related to lack of exposure/recall, information misinterpretation, possibly evidenced by questions, statement of concern, and inaccurate follow-through of instruction/development of preventable complications.
4. Disturbed Body Image may be related to biophysical changes (presence of stoma; loss of control of bowel elimination) and psychosocial factors (altered body structure, disease process/associated treatment regimen, e.g., cancer, colitis), possibly evidenced by verbalization of change in perception of self, negative feelings about body, fear of rejection/reaction of others, not touching/looking at stoma, and refusal to participate in care.
5. Impaired Social Interaction may be related to fear of embarrassing situation secondary to altered bowel control with loss of contents, odor, possibly evidenced by reduced participation and verbalized/observed discomfort in social situations.
6. Risk for Sexual Dysfunction: risk factors may include altered body structure/function, radical resection/treatment procedures, vulnerability/psychologic concern about response of SO(s), and disruption of sexual response pattern (e.g., erection difficulty)
Nursing Diagnois for Hyperthermia related to Tetanus. Nursing Interventions related to Hyperthermia related to Tetanus
Hyperthermia
Hyperthermia is an elevated body temperature due to failed thermoregulation. Hyperthermia occurs when the body produces or absorbs more heat than it can dissipate. When the elevated body temperatures are sufficiently high, hyperthermia is a medical emergency and requires immediate treatment to prevent disability or death.
The most common causes are heat stroke and adverse reactions to drugs. Heat stroke is an acute condition of hyperthermia that is caused by prolonged exposure to excessive heat or heat and humidity. The heat-regulating mechanisms of the body eventually become overwhelmed and unable to effectively deal with the heat, causing the body temperature to climb uncontrollably. Hyperthermia is a relatively rare side effect of many drugs, particularly those that affect the central nervous system. Malignant hyperthermia is a rare complication of some types of generahttp://www.blogger.com/img/blank.gifl anesthesia.
Hyperthermia can be created artificially by drugs or medical devices. Hyperthermia therapy may be used to treat some kinds of cancer and other conditions, most commonly in conjunction with radiotherapy.
Hyperthermia differs from fever in the mechanism that causes the elevated body temperatures: a fever is caused by a change in the body's temperature set-point.
The opposite of hyperthermia is hypothermia, which occurs when an organism's temperature drops below that required for normal metabolism. Hypothermia is caused by prolonged exposure to low temperatures and is also a medical emergency requiring immediate treatment. ncp-blog.blogspot.com
1. Set the temperature a comfortable environment. Rational: climate and environment can affect an individual's body temperature as a process of adaptation through the process of evaporation and convection.
2. Monitor body temperature every two hours. Rational: identification of developmental symptoms of exhaustion towards the shock.
3. Provide adequate hydration or drinking. Rational: fluids help refresh the body and is a compressed body of a fever.
4. Take action aseptic and antiseptic techniques in wound care. Rational: eliminate the possibility of toxin treatment of wounds that are still located around the wound.
5. Give cold compress when no external stimuli seizures. Rational: cold compress is one way to lower body temperature by means of conduction process.
6. Implement program of antibiotics and antipyretic treatment. Rational: the drugs may have antibacterial spectrum to treat gram-positive or gram-negative bacteria, antipyretic worked as a process of thermoregulation to anticipate the heat.
7. Collaboration in the laboratory examination of leukocytes. Rational: the results of leukocytes increased by more than 100.000/mm3 identify an infection and or to keep abreast of the prescribed treatment.
Ineffective Breathing Pattern is a condition that poses significant challenges to individuals and requires targeted nursing interventions to optimize respiratory function. Nursing care plays a pivotal role in identifying the underlying causes, managing symptoms, and promoting effective breathing patterns. This article explores various nursing interventions aimed at addressing Ineffective Breathing Pattern, emphasizing a comprehensive and patient-centered approach.
Assessment and Monitoring
The foundation of nursing interventions for Ineffective Breathing Pattern lies in a thorough assessment of the patient's respiratory status. Nurses routinely monitor vital signs, such as respiratory rate, depth, and rhythm, to identify deviations from normal patterns. Additionally, assessing the patient's overall lung function, chest movement, and oxygen saturation levels provides valuable information for tailoring interventions.
Collaboration with Healthcare Team
Effective nursing care involves collaboration with other healthcare professionals, including respiratory therapists, physicians, and pharmacists. Open communication ensures a comprehensive understanding of the patient's medical history, current medications, and ongoing treatment plans. Collaborative efforts facilitate a holistic approach to care, addressing both the immediate symptoms and the underlying causes of Ineffective Breathing Pattern.
Oxygen Therapy
For individuals experiencing respiratory distress or hypoxia, oxygen therapy is a fundamental nursing intervention. Nurses assess oxygen saturation levels using pulse oximetry and administer supplemental oxygen as prescribed. Ensuring appropriate oxygen delivery supports optimal gas exchange, alleviates symptoms, and prevents further respiratory compromise.
Positioning Techniques
Strategic positioning is an essential nursing intervention to enhance respiratory function. For patients with Ineffective Breathing Pattern, optimal positioning includes elevating the head of the bed to promote lung expansion and reduce the work of breathing. Additionally, side-lying positions or specific postural adjustments may improve ventilation and facilitate effective breathing.
Breathing Exercises and Techniques
Nurses play a crucial role in teaching and encouraging patients to perform breathing exercises and techniques. Deep breathing exercises, pursed-lip breathing, and diaphragmatic breathing can enhance lung expansion and strengthen respiratory muscles. These exercises empower patients to actively participate in their care, promoting a sense of control over their breathing patterns.
Respiratory Therapy
Collaborating with respiratory therapists allows nurses to implement specialized interventions such as nebulizer treatments, chest physiotherapy, and incentive spirometry. These therapies aid in clearing airway secretions, promoting effective coughing, and improving overall lung function. Consistent monitoring and documentation of the patient's response to respiratory therapy guide ongoing care adjustments.
Patient Education
Empowering patients with knowledge about their respiratory condition is a cornerstone of nursing interventions. Educating patients about the importance of medication compliance, proper inhaler technique, and recognizing early signs of respiratory distress enables them to actively engage in their care. Patient education fosters a sense of partnership between the patient and the healthcare team, contributing to long-term respiratory well-being.
Anxiety Management
Ineffective Breathing Pattern can be exacerbated by anxiety and stress. Nursing interventions include implementing strategies to alleviate anxiety, such as therapeutic communication, relaxation techniques, and creating a calm environment. Addressing the emotional aspect of respiratory distress contributes to a more holistic approach to care.
Environmental Modifications
Nurses assess the patient's environment to identify and eliminate factors that may contribute to Ineffective Breathing Pattern. Ensuring proper ventilation, controlling allergens or irritants, and maintaining a comfortable temperature support respiratory well-being. Patient comfort is paramount, and environmental modifications contribute to overall care efficacy.
Evaluation and Adjustment of Care Plan
Ongoing evaluation of nursing interventions is essential to gauge their effectiveness and make necessary adjustments to the care plan. Regular assessments of respiratory status, vital signs, and patient-reported symptoms guide modifications to medication regimens, positioning strategies, and breathing exercises. Collaboration with the healthcare team ensures a dynamic and responsive approach to patient care.
Bibliography :
1. Black, J. M., & Hawks, J. H. (2009). Medical-surgical nursing: Clinical management for positive outcomes. Saunders/Elsevier.
2. Peate, I. (2016). Fundamentals of nursing. John Wiley & Sons.
3. Hough, A. (2018). Physiotherapy in Respiratory and Cardiac Care: An Evidence-Based Approach. Cengage Learning.